The Ministry of Health and Social Development of Mali has been using the DHIS2 platform for Health Information System data management at all levels since 2016. It has been a priority to improve data reporting and real-time decision-making in the country.
The DHIS2 platform hosts aggregate and individual data on priority diseases suspected and confirmed cases, as well as deaths. There is a system update each time an emerging or re-emerging disease is the subject of priority surveillance in Mali, like what happened during the COVID-19 pandemic. Even so, real-time data entry in DHIS2 has remained timid with low quality regarding completeness, timeliness, accuracy, and consistency.
Mali integrated COVID-19 into its epidemiological alert system and parameterized it in the DHIS2 platform very early into the pandemic, which aimed to facilitate real-time decision-making in the country. The Government promoted capacity building for system users, who also received tablets for entering aggregated and individual data to inform the national response to the virus.
However, there were challenges regarding data availability and access, as well as information sharing. Primary source data registries were fragmented and did not involve all Health Information System actors.
Epidemic waves have often affected the entire health system in Mali, particularly when it comes to regular data entry. It was no surprise that health facilities were quickly overwhelmed by the large amount of individual data produced in 2020, 2021 and the first quarter of 2022 due to the COVID-19 pandemic.
To help address these bottlenecks, CHISU carried out a rapid assessment to identify the shortcomings that were hampering the epidemiological alert system set up in response to the COVID-19 epidemic.
The assessment helped identify human resources challenges and data entry shortcomings in the DHIS2 COVID module, including access to Internet connection packages, tablet updates and data synchronization problems.

Other issues identified included poor supervision, routine control and data quality review. There was also insufficient partner coordination during the implementation of activities to strengthen Mali’s Health Information System.
CHISU defined priority intervention areas to improve the availability of quality data in the DHIS2 COVID-19 tracker. For a whole month, motivated data entry officers carried out historical surveillance entries covering 2020-2022. Officers also received a refresher training on how to enter data into the DHIS2 COVID-19 tracker.

The establishment of WhatsApp groups by region, a quality control group at the central level, monthly meetings and the revitalization of quarterly reviews were some of the other initiatives that help improve data quality in Mali.
"With CHISU support, we were able to raise the availability and quality of COVID-19 data; we feel more accountable now," said Nattan Sawagodogo, a data manager from Bamako.

Each data entry officer received a monthly stipend for Internet connection that allowed for remote monitoring through a WhatsApp group, supplemented with regular supervisory visits to health facilities.
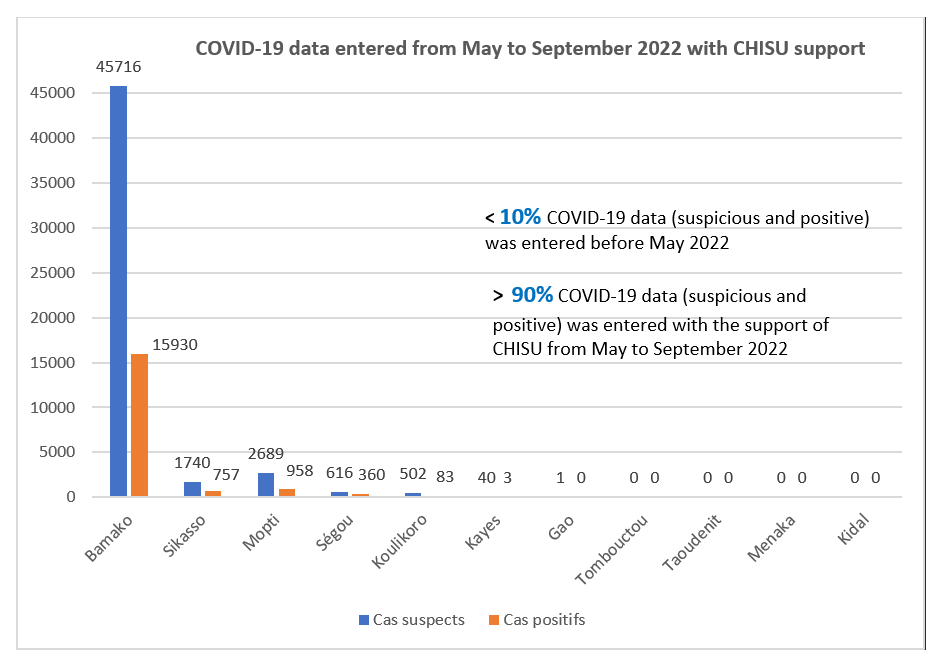
Before CHISU, district-level data did not allow for indicator monitoring or decision-making due to low quality. “Despite ongoing data entry efforts, we are seeing a significant improvement in data availability in DHIS2 in the regions supported by the program: Bamako, Sikasso, Segou and Mopti,” said Mr. Sawagodogo.
As of October 2022, historical COVID-19 surveillance data registered through DHIS2 was above 90%, clearing the backlog from previous years, when there was less than 10% of surveillance data registered through the platform.
Moving forward, CHISU will explore the inclusion of other priority regions and commitment by partners to improve quality data from the COVID-19 response. “In the event of an epidemic wave, this will ensure we have the ability to enter data in real time at the health facilities level,” Mr. Sawagodogo added.